Cholangiocarcinoma
The Common Vein Copyright 2008
Cholangiocarcinoma is a malignant proliferation of the epithelial lining of the intrahepatic or extrahepatic bile ducts. It is the second most common primary liver malignancy.
The reported incidence of cholangiocarcinoma in the US is 1-2 cases per 100,000 patients. The peak incidence occurs in the seventh decade of life.
Primary sclerosing cholangitis is the most common predisposing factor . Unresected congenital biliary cysts, liver flukes and thorotrast exposure are other identified risk factors for cholangiocarcinoma.
Pathology : Geographically 60 – 70 % of cholangiocarcinomas occur at the confluence of the right and left hepatic ducts, 20-30%at the distal common bile duct and 5-15% within the liver. Morphologically intrahepatic and extrahepatic tumors are classified (Liver Cancer Study Group of Japan) according to their growth characteristics (1) mass forming (2) periductal infiltrating and (3) intraducatal growing.
Microscopy: Cholangiocarcinomas are adenocarcinomas and thus show glandular features .
Clinical presentation and Physical findings:
Symptoms vary based on the location and size of the tumor. Dull pain in the right upper quadrant, anorexia, weight loss and very rarely jaundice are presenting symptoms of intrahepatic cholangiocarcinomas. On the other hand painless jaundice is the most common presentation of extrahepatic tumors. The gall bladder may be palpable in cases extrahepatic cholangiocarcinomas caused by obstruction at or distal to the origin of the cystic duct (Courvoisier law).
Diagnosis:
Laboratory studies show an obstructive picture with increased direct billirubin, increased alkaline phosphatase and increased gama glutamyl transpeptidase.
Imaging studies are the initial first step in diagnosis. Ultrasound may intrahepatic bile duct dilatation with normal extrahepatic ducts in patients with proximal (hilar) lesions, or dilation of both intrahepatic and extrahepatic ducts in more distal lesions.
CT – triple phase and MRI provide further information regarding extent and respectability of the tumor . High quality MR is the optimal imaging technique to determine extent of the disease .
ERCP , MRCP and endoscopic ultrasound may be helpful in early cholangiocarcinoma, where CT and MRI may be negative . ERCP also provides a means of tissue sampling for biopsy, therapeutic decompression where there is cholangitis and the option of stenting for palliation in unresectable tumors.
Staging and Treatment – Trratment modalities depend on accurate staging . Staging is done by tumor, node , metastasis – TNM staging. Laproscopy to detect peritoneal or superficial metastasis may be a part of staging for resectable early cholangiocarcinoma .
Definitive therapy involves surgical resection but is possible in only a few patients due to advanced disease at presentation . Liver transplantation is contraindicated unlike HCC , due to increased recurrence rates of cholangiocarcinoma . Palliative options include stenting , chemotherapy and radiation .
Since this presentation is about liver tumors, the focus is on the least common tumors of biliary origin which are the intrahepatic cholangiocarcinomas. They represent the second most common primary tumors of the liver. Intrahepatic cholangiocarcinomas (ICC) are relatively rare and account for 5-15% of the bile duct tumors, and account for only 7% of liver tumors in the US.
There both scirrhous and non scirrhous types. The scirrhous types have more fibrous tissue with a poorer prognosis, probably due to the desmoplastic nature of the fibrous tissue.
The imaging purpose is to differentiate ICC from an HCC or from other malignant tumors of the liver.
CT of ICC shows homogeneous hypodense mass with peripheral enhancement that tends to fill in on 4-6 minute delay. ( Maetani) In the presence of necrosis, no ehancement is noted. The desmoplastic nature can result in capsular retraction. Associated findings include dystrophic calcification, satellite nodules, and peripheral intrahepatic duct dilatation (Chung) Since the fibrosis is mostly central, it is characteristic for the center of tumor to show hypointensity on T2. The fibrotic tissue also manifests with delayed enhancement and thus the combination of these two findings of central low intensity on T2 and delayed enhancement together with peripheral duct ectasia, are characteristic
|
Intrahepatic Cholangiocarcinoma |
| The CT shows the appearance of a cholangiocarcinoma on a 3 phase liver protocol. On the non contrast study (a) the mass in the dome of the liver shows infiltrative pattern with faint central calcification. In the arterial phase (b), there is heterogenous arterial staining. On the delayed phase more intense enhancement is noted. The heterogeneity suggests a combination of fibrotic tissue and non fibrotic or necrotic tissue. Image d, is a transverse from a more caudal aspect and shows a dilated bile duct (white arrow), and extension of the tumor more inferiorly (black arrow).
code liver hepatic mass cancer calcification intrahepatic cholangiocarcinoma enhancement CTscan copyright 2009 Courtesy Ashley Davidoff MD all rights reserved 18126cb02.8s |

|
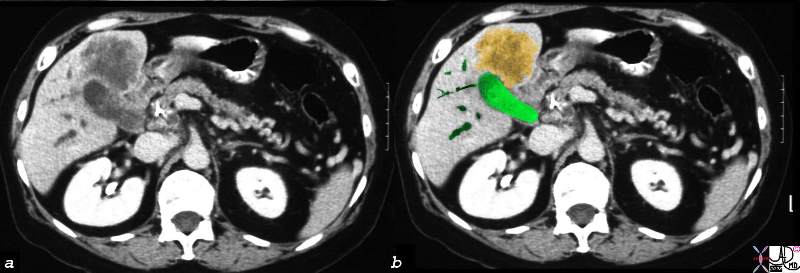
Gallbladder Cholangiocarcinoma |
| 16254c02b.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008 |
Cholangiocarcinoma is an uncommon malignant growth of the epithelial lining of the bile duct of unknown cause resulting in a mass that presents in the liver or in the extrahepatic bile ducts.
|
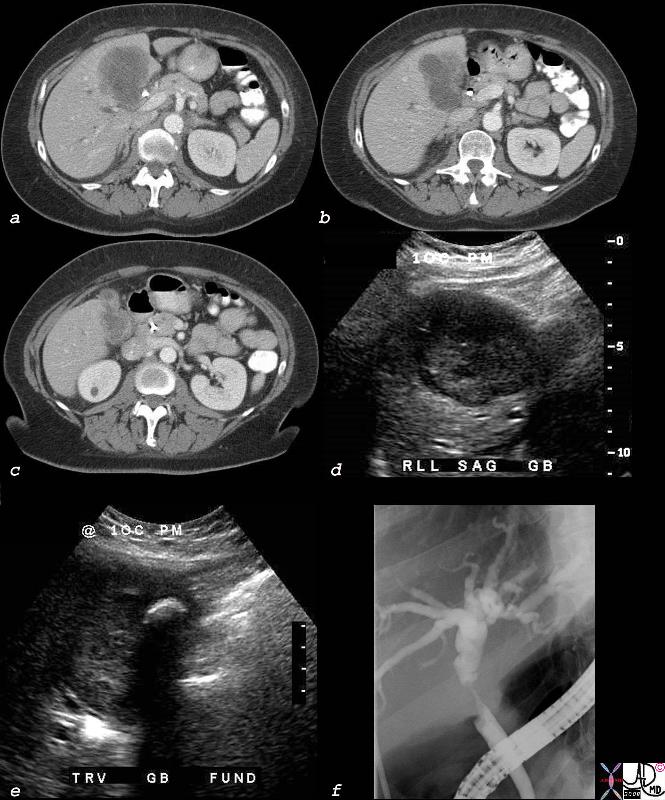
Cholangiocarcinoma with Involvement of the Gallbladder and Bile Duct |
| 40018c01b.8s elderly female cholelithiasis obstructive jaundice common bile duct stricture dilated intrahepatic ducts irregular enhancing thickening of the gallbladder wall stent gallbladder carcinoma with extension into the CBD or CBD carcinoma with extension into the wall of the gallbladder CTscan USscan ultrasound ERCP Courtesy Ashley DAvidoff MD copyright 2008 |
|
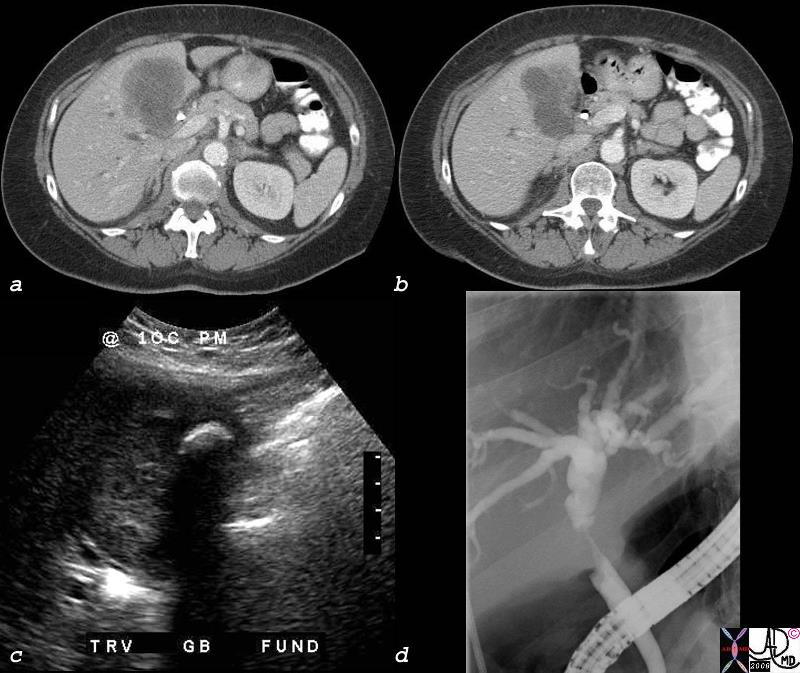
Cholangiocarcinoma with Involvement of the Gallbladder and Bile Duct |
| 40018c02b.8s elderly female cholelithiasis obstructive jaundice common bile duct stricture dilated intrahepatic ducts irregular enhancing thickening of the gallbladder wall stent gallbladder carcinoma with extension into the CBD or CBD carcinoma with extension into the wall of the gallbladder CTscan USscan ultrasound ERCP Courtesy Ashley DAvidoff MD copyright 2008 |